What is Diabetic Retinopathy?
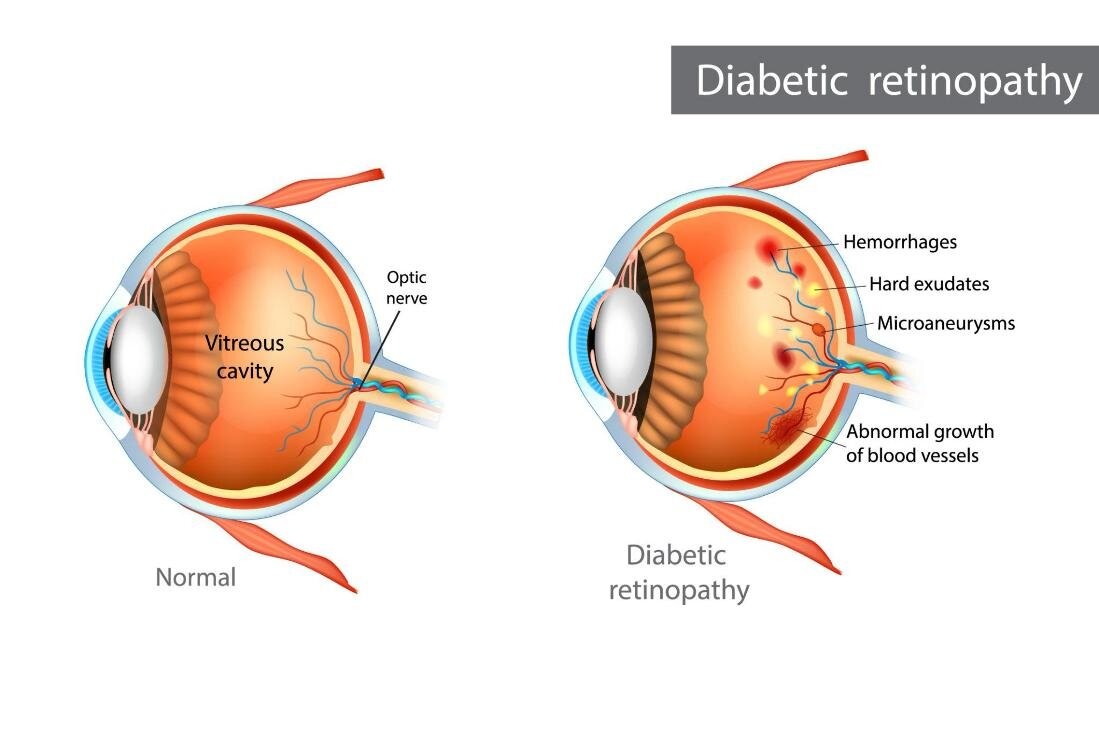
Diabetic retinopathy (DR) is a microvascular complication of diabetes mellitus (both type 1 and type 2) in which chronically elevated blood sugar levels damage the small blood vessels that supply the retina. The disease progresses through stages, beginning with non-proliferative diabetic retinopathy (NPDR), in which the retinal capillaries weaken, develop microaneurysms, leak fluid and blood, and may become occluded. As the disease advances to proliferative diabetic retinopathy (PDR), the retina responds to widespread ischemia by growing new, abnormal blood vessels (neovascularization). These fragile vessels are prone to hemorrhage, which can cause vitreous hemorrhage and tractional retinal detachment — potentially devastating complications. Diabetic macular edema (DME), the accumulation of fluid in the macula, can occur at any stage and is the most common cause of vision loss in diabetic patients. The risk of developing DR increases with the duration of diabetes: after 20 years, nearly all type 1 and over 60% of type 2 diabetic patients will have some degree of retinopathy.
Symptoms
- Often asymptomatic in the early stages — underscoring the need for regular screening
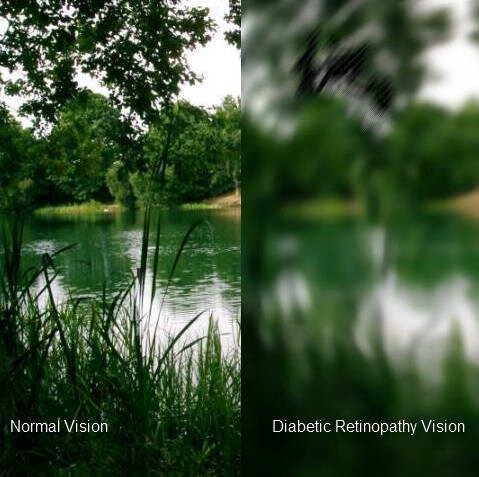
- Blurred or fluctuating vision
- Floaters (dark spots or strings drifting in the visual field)
- Dark or empty areas in the visual field
- Difficulty with color perception
- Sudden severe vision loss (vitreous hemorrhage or retinal detachment)
- Distorted central vision (macular edema)
Causes and Risk Factors
The fundamental cause is chronic hyperglycemia, which triggers a cascade of biochemical and cellular changes in the retinal vasculature, including pericyte loss, basement membrane thickening, endothelial cell damage, and breakdown of the blood-retinal barrier. Key risk factors include:
- Poor glycemic control (elevated HbA1c)
- Duration of diabetes — the single most important predictor
- Hypertension
- Dyslipidemia (elevated cholesterol and triglycerides)
- Pregnancy (can accelerate retinopathy progression)
- Smoking
- Chronic kidney disease (diabetic nephropathy)
- Rapid improvement in glycemic control after prolonged poor control (early worsening phenomenon)
Diagnosis
Screening and diagnosis are performed through a dilated fundus examination. The ophthalmologist looks for microaneurysms, dot and blot hemorrhages, hard exudates, cotton-wool spots, venous beading, intraretinal microvascular abnormalities (IRMA), and neovascularization. OCT is essential for detecting and quantifying diabetic macular edema. Fluorescein angiography maps areas of capillary non-perfusion, leakage, and neovascularization. OCT angiography (OCTA) is an emerging non-invasive alternative for visualizing the retinal vasculature. Ultra-widefield fundus photography allows assessment of peripheral retinal changes. International guidelines recommend annual dilated eye examinations for all diabetic patients, beginning at diagnosis for type 2 and within 5 years of diagnosis for type 1.
Treatment
Treatment depends on the stage and presence of macular edema:
- Systemic management — tight glycemic control (HbA1c target below 7%), blood pressure control, and lipid management are foundational and can significantly reduce the risk and progression of retinopathy
- Intravitreal anti-VEGF therapy — first-line treatment for center-involving diabetic macular edema and PDR; agents include ranibizumab, aflibercept, and faricimab
- Intravitreal corticosteroid implants — dexamethasone (Ozurdex) or fluocinolone acetonide (Iluvien) for DME, particularly in pseudophakic patients or those not responding to anti-VEGF
- Panretinal photocoagulation (PRP) — laser treatment applied to the peripheral retina to reduce neovascularization in PDR
- Focal/grid laser photocoagulation — for non-center-involving macular edema
- Vitrectomy — surgical removal of the vitreous gel for non-clearing vitreous hemorrhage, tractional retinal detachment, or combined tractional-rhegmatogenous detachment
Prevention and Recommendations
- Maintain optimal blood sugar levels as directed by your endocrinologist or diabetologist
- Control blood pressure and cholesterol through lifestyle and medication
- Attend annual dilated eye examinations without fail
- Do not skip screening even if your vision feels normal — early stages are often symptom-free
- Stop smoking
- Exercise regularly and maintain a healthy body weight
- Report any new visual symptoms (floaters, blurring, dark spots) to your ophthalmologist immediately
- Women with diabetes should have an eye examination before or early in pregnancy and be monitored throughout